


1Department of Dermatology, Osaka National Hospital, 2-1-14 Hoenzaka Chuo-ku, Osaka 540-0006, 2Tanii Dermatology Clinic, 3Department of Dermatology, Osaka City University Graduate School of Medicine, Osaka, and 4Department of Dermatology, Kurume University School of Medicine, Kurume, Japan. *E-mail address: ozawa.kentaro.kj@mail.hosp.go.jp
Accepted Sep 12, 2019; E-published Sep 12, 2019
The aetiology of Grover’s disease, which was initially described by Grover in 1970 as transient acantholytic dermatosis, is unknown. Although the disease typically resolves within 6–12 months, it can persist for several years. We report here an atypical and unique case of persistent Grover’s disease that presented with predominant bullous skin lesions with neutrophil-rich infiltration.
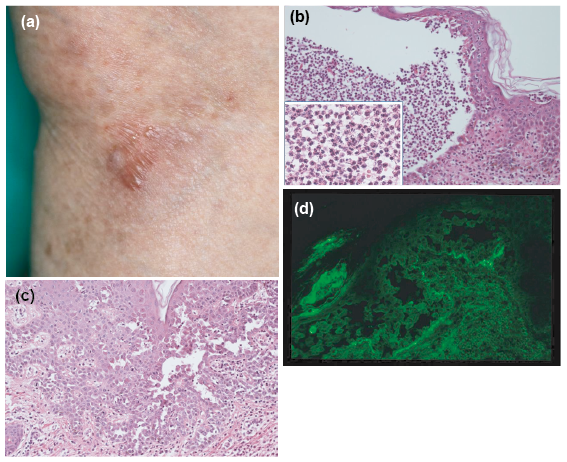
A 77-year-old Japanese woman was referred to our department in June 2012 because of multiple pruritic bullae and vesicles surrounded by minor erythema on the trunk and limbs (Fig. 1a), which had initially developed 2 months earlier. She had been treated with topical corticosteroids, which resulted in temporary and moderate relief. Laboratory blood test results revealed an unremarkable haematological profile. Enzyme-linked immunoassay (ELISA) tests for antibodies to desmoglein 1, desmoglein 3 and BP180 were all negative. Moreover, bacterial culture of the blister content was negative. Initial biopsy of the vesicle on the chest revealed an intraepidermal blister containing acantholytic cells and substantial neutrophil accumulation (Fig. 1b). Neutrophilic infiltration was also seen in the papillary dermis. Acantholytic suprabasal clefts with dyskeratotic cells were noted at different sites on the same specimen (Fig. 1c). Direct immunofluorescence microscopy did not reveal deposition of immunoglobulin (Ig)G, IgM, IgA, C3 or fibrinogen.
Based on these findings, the patient was diagnosed with Grover’s disease. She was administered minocycline (200 mg/day), which resulted in rapid regression of the eruption. However, discontinuation of minocycline resulted in recurrence of Grover’s disease.
Thereafter, she had repeated remissions and recurrences for 3 years. In August 2015, a second biopsy of the buttock revealed a pemphigus-like acantholytic suprabasal cleft with focal dyskeratosis in the epidermis. Direct immunofluorescence microscopy revealed linear and granular deposition of C3 in the basement membrane (Fig. 1d). Serological studies, including indirect immunofluorescence microscopy, ELISA and immunoblotting, showed negative results. Following the second biopsy, treatment with minocycline (100 mg/day) was reinitiated, and the eruption resolved within 3 days. Thereafter, there was no recurrence of Grover’s disease, even after the discontinuation of minocycline treatment in January 2017.
Fig. 1. Clinical, histopathological and direct immunofluorescence microscopic findings in the present patient. (a) Clinical features at first visit. (b) Histopathological findings with massive neutrophilic infiltrate in the epidermis (haematoxylin and eosin (HE) ×100; ×400 inset). (c) Histopathological evaluation showed suprabasal acantholytic cleft and dyskeratosis (HE ×100). (d) Results for C3 deposition in the second biopsy.
Grover’s disease typically resolves within 6–12 months; thus, it is termed transient acantholytic dermatosis. The persistent nature of the disease in the present case corresponds to the variant “persistent acantholytic dermatosis”, named by Simon et al. (1)
The present case was unique in having prominent bullous lesions surrounded by minimal erythema and neutrophil-rich infiltration. Bullous lesions have been reported as a rare clinical variant of Grover’s disease, although their clinical significance remains unknown (2, 3). Recently, Fernandez-Figueras et al. conducted a histopathological analysis of cases of Grover’s disease and demonstrated an abundant neutrophilic infiltration in 5% of examined cases (4). We suggest that the current case corresponds to this neutrophil-rich variant. Furthermore, the effectiveness of minocycline may be associated with the predominant neutrophilic infiltration observed because of its anti-inflammatory and anti-leukochemotactic activities (5).
We examined the possibility of the development of autoimmune bullous disease in our patient because she persistently presented with new bullous lesions for >3 years. Extensive examinations for various autoimmune bullous diseases showed no positive results, which was consistent with the diagnosis of Grover’s disease. The significance of the linear and granular deposition of C3 in the second biopsy remains unclear. However, this finding may be related to the pathomechanisms in granular C3 dermatosis, which we recently proposed as a possible novel disease entity (6). In conclusion, we report here a case of neutrophil-rich variant of persistent bullous Grover’s disease, which was treated effectively with minocycline.
The authors would like to thank Enago (www.enago.jp) for English language review.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize